Three Positions, Three Outcomes
Where you seat the implant shoulder relative to the bone crest determines what happens at the microgap — and what happens at the microgap determines whether bone is preserved or lost.
Dr. Farid Ebrahim breaks down each positioning philosophy, what the evidence supports, and where the science draws a hard line.
This is not a minor detail. It is the whole game.

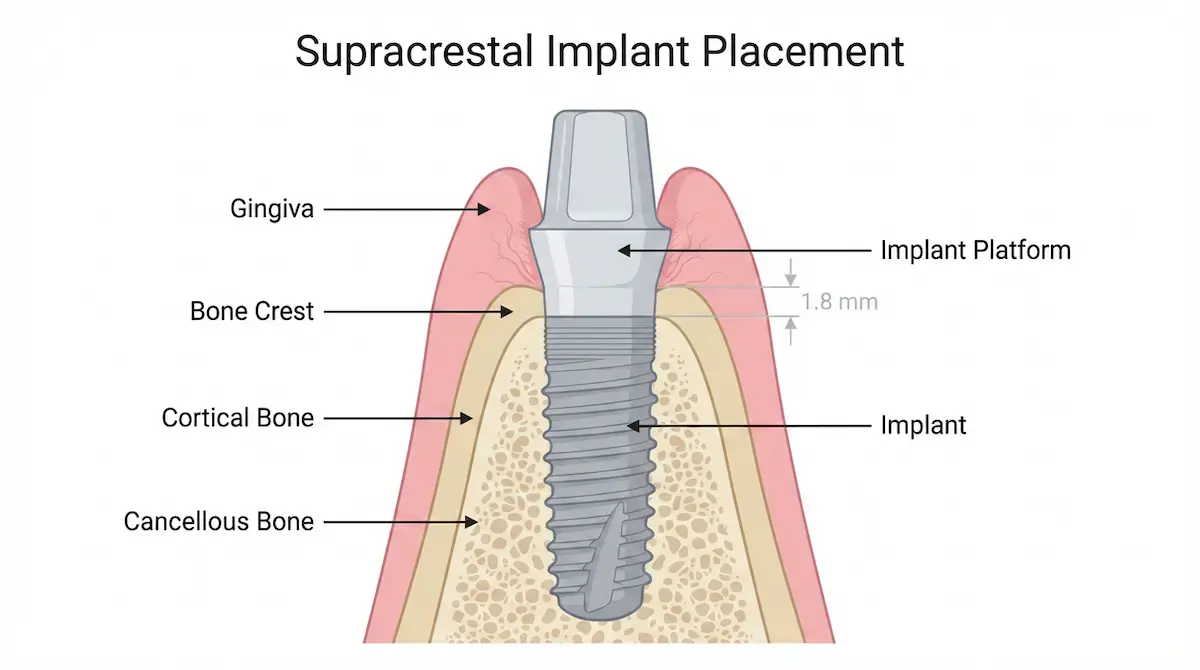
1. Supracrestal Placement
(Tissue-Level)
The implant shoulder (platform) sits above the bone crest. The microgap — the junction between implant and abutment where bacteria is extruded from the internal aspect of the implant due to micro movement — is positioned away from the bone entirely.
This is the tissue-level philosophy. By elevating the microgap above the crestal bone, you remove the source of chronic peri-implant inflammation from the one place it does the most damage.
The science supporting supracrestal placement is well-established. For clinicians working with tissue-level systems, this positioning is predictable and forgiving across biotype variations.
"That being said, we try to minimize the use of tissue-level implants with polished collars unless we have no other choice."
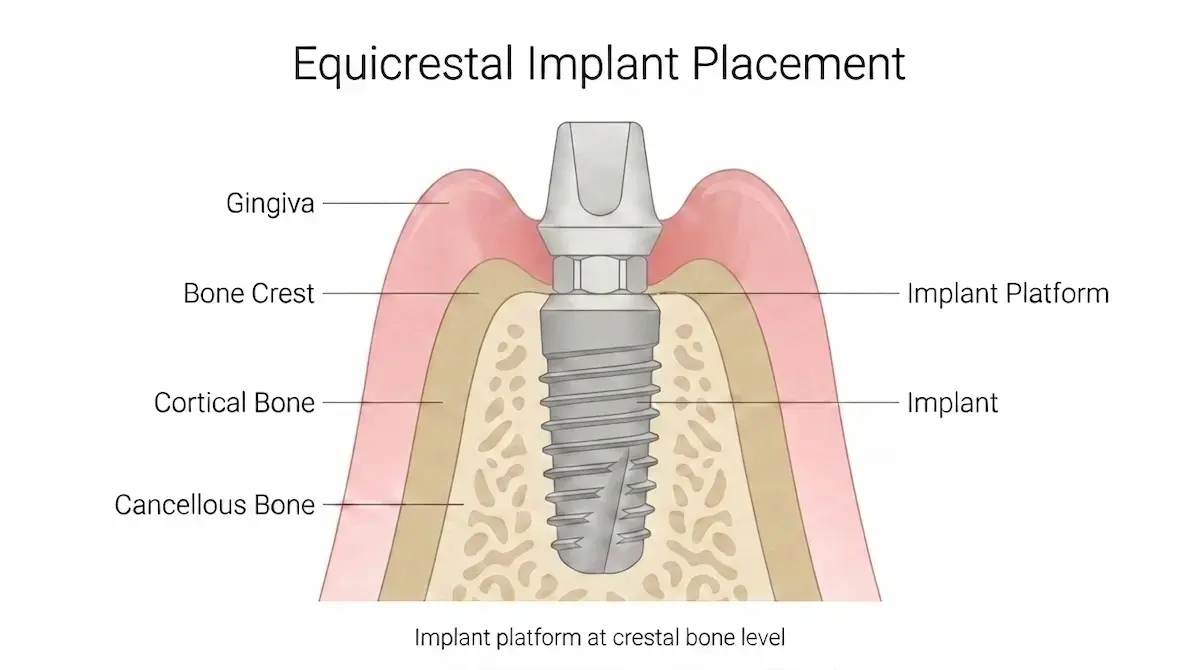
2. Equicrestal Placement
(Bone-Level Flush)
The implant shoulder sits flush with the bone crest. For decades, the marginal bone loss that followed was considered a normal biological response — an acceptable cost of integration.
It was not normal. It was preventable.
The microgap sitting at bone level creates a low-grade, chronic inflammatory environment. In patients with thin gingival biotype — less than 3mm of tissue above the boney crest — this results in saucerization: 360-degree bone loss to below the implant platform.
Thin tissue offers less protection. The bone responds, and loss compounds over time.
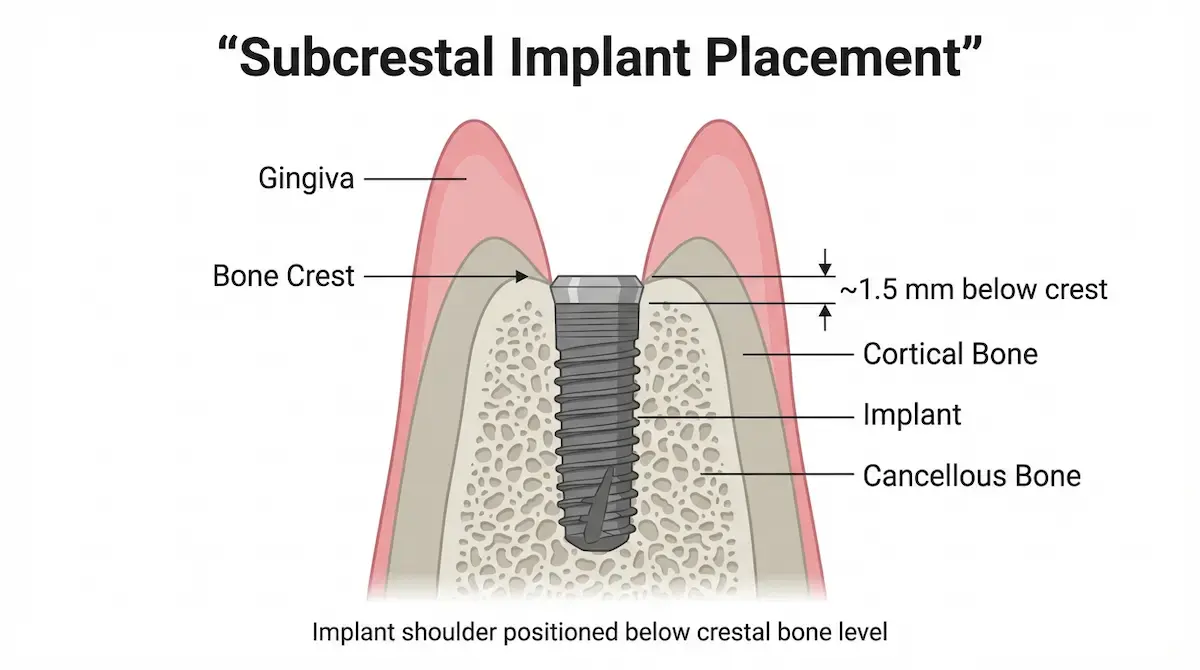
3. Subcrestal Placement
(Bone Crest Level)
The implant shoulder is placed below the bone crest, burying the microgap beneath bone.
When executed correctly — with platform switching and a morse-cone internal connection — the conical taper creates what is effectively a cold weld. Bacterial leakage approaches zero. Micromotion is significantly reduced. Bone does not just tolerate the implant; it migrates over the shoulder.
This is the principle behind zero bone loss implants — not a marketing claim, but a measurable outcome driven by connection geometry and surgical positioning.
The critical caveat: Subcrestal placement only works with morse-cone connection and platform switching.
With an external hex attachment, the microgap is wide and the components flex under load — pumping bacteria directly into the bone with every occlusal cycle. That is why external hex attachments are not recommended for subcrestal placement.
The depth that protects with one connection type destroys with another.
The Rules That Follow From the Evidence
Connection type determines everything about implant placement depth decisions. The position you choose must match the connection you are working with.
Supracrestal: Supported by strong evidence across connection types. Reliable, particularly for tissue-level systems.
Subcrestal: Morse-cone connections only. If you are working with an external hex, do not go sub-crestal.
One abutment, one time. Every disconnection of the abutment disrupts the soft tissue seal that formed during healing. Bone migrates apically in response. The zero bone loss outcome depends on not repeating this step.
ISQ below 60: Do not attempt subcrestal placement. Stability is insufficient. Go two-stage, allow undisturbed healing, and reassess integration before loading.
What This Means Clinically
Placement depth is not a preference. It is a decision with biological consequences tied directly to connection geometry. The microgap position dictates the inflammatory environment, and the connection type dictates whether that environment is sealed or open.
For clinicians placing implants, the takeaway is clear: know your connection, know your biotype, and position accordingly.
Final Thoughts
The connection type you select and the depth you place are not independent choices. They are two variables in the same equation. Get both right and the bone responds accordingly.
The 3rdSET hands-on implant course applies evidence-based placement protocols — including Zero Bone Loss concepts — across real surgical cases with direct faculty mentorship.
View available course dates and registration at www.3rdsetce.com/implant-courses.
Dr. Farid Ebrahim is a course director at 3rdSET, where general dentists train on live-patient implant surgeries in a 4-day mini-residency format.